I’m writing a book about reverse psychology; please don’t buy it.
This one’s not by Rappaport
The judge said I had to keep 6 feet away from my ex-wife. So I buried her under the patio.
Robert Buxbaum: the above 3 jokes are from Jack Rappaport — He sometimes sells jokes. April 13, 2022. The ones below are from Gahan Wilson, and the one at right, I don’t know.
In this blog-post, I’d like to report on the first random study of patients with Atrial fabulation, A-Fib, and sleep apnea, comparing the health outcome of those who use a C-PAP, a “Continuous Positive Airway Pressure” device, to the outcome those who do not. The original study was published in May, 2021 (read it here) in the American Journal of Respiratory and Critical Care Medicine. The American Journal, Pulmonary Advisor published a more-popular version here.
As a background, if you are over 65 and overweight, there is a 25% chance or so that your heart rate will begin to surge semi-randomly, and that it will flutter. This is Atrial fabulation, A-Fib. It tends to get worse and tends to lead to heart attacks and strokes. People with A-fib tend to be treated with drugs, aspirin, warfarin, beta blockers, and anti arrhythmics. They also tend to be prescribed a C-PAP because overweight, older folks tend to snore and wake up a lot during the night (several times per hour: apnea).
A C-PAP definitely stops the snoring and the Apnea, and the assumption was that it would help your heart as well, if only by giving you a better night’s sleep. As it turns out, the C-PAP seems to decrease heart health — significantly.
For this study, adult patients between 18 and 75 years old diagnosed with paroxysmal A-Fib (that’s occasional AF) were screened for moderate to severe sleep apnea. Those who agreed to participate were randomly assigned to either a treatment of C-PAP plus usual care (drugs mostly) or just usual care for the next 5 months. Of the 109 who enrolled in the study, 55 got the C-PAP plus usual care, 54 got usual care alone. The outcome was that there were 9 serious, adverse heart events (strokes and heart attacks); 7 were in the C-PAP group.
The CPAP pressure was, on average, 6.8 cm H2O; mean time of use was 4.4±1.9 hours per night. The C-PAPs did their jobs on the apnea too, reducing residual apnea-hypopnea to 2.3±1.9 events per hour for those in the C-PAP group.
There was a non-statistically significant reduction is AF among the C-PAP group. They reduced their time in AF by 0.6 percentage points compared to the control group (95% CI, -2.55 to 1.30; P =.52). That not a statistically significant difference, and is most likely random.
There was a statistically significant decrease in heart health, though. A total of 7 serious adverse events occurred in the C-PAP group and only 2 in the control group. A total of 9 is a relatively small number of events, but there is a strong statistical difference between 7 and 2.
The authors conclude: “CPAP treatment does not seem to reduce or prevent paroxysmal AF.” They should also have concluded that it reduced heart health with a statistical confidence of ~82%: (1-2(36+10)/512) =82%. See more on this type of statistics.
A possible explanation of why a C-PAP would would make heart health worse is an outcome of the this recent sleep study (link here). It appears that the C-PAP helps restore breathing, but by doing so, it interferes with a mechanism the body uses to deal with A-fib. It seems that, for people with A-Fib, their bodies use breathing stoppages to get their heart back into rhythm. For these people, many of their breathing stoppage are not obstructive, but a bio-pathway to raise the CO2 level in the blood and thus regulate heart rate. The use of a C-PAP prevents this restorative mechanism and this seem to be the reason it is destructive to the heart-health of patients with A-fib. On the other hand, a C-PAP does improve the sleep those patients whose apnea is obstructive. It seems to me that sleep studies should do a better job distinguishing the two causes of apnea. C-PAPs seem counter-indicated for patients with A-fib.
Robert Buxbaum, March 30, 2022. I was diagnosed with apnea and A-Fib some years ago. The sleep doctor prescribed a C-PAP and was adamant that I had to use it to keep my heart healthy. There were no random studies backing him up or contradicting him until now.
With the sun setting earlier, and the threat of new COVID lockdowns, there is a real threat of a depression, seasonal and isolation. A partial remedy is exercise; it helps fight depression whether you take other measures not. An article published last month in the Journal of Affective Disorders reviewed 22 studies of the efficacy of exercise, particularly as an add-on to drugs and therapy. Almost every study showed that exercise helped, and in some studies it helped a lot. See table below. All of the authors are from the University of British Columbia. You can read the article here.
From “Efficacy of exercise combined with standard treatment for depression compared to standard treatment alone: A systematic review and meta-analysis of randomized controlled trials.” by JacquelineLee1 et al.In virtually every study, exercise helps fight depression.
For those who are willing to exercise, there are benefits aside from mental health. Even a daily walk around the block helps with bone strength, weight control, heart disease, plus the above mentioned improvement in mood. More exercise does more. If you bicycle without a helmet, you’re likely to live longer than if you drive.
For those who can’t stand exercise, or if exercise isn’t quite enough to send away the blues, you can try therapy, medication, and/or diet. There is some evidence that food that are high in lithium help fight depression. These food include nuts, beans, tomatoes, some mineral waters, e.g. from Lithia springs, GA. The does is about 1/100 the dose given as a bipolar treatment, but there is evidence that even such small doses help. Lithium was one of the seven ingredients in seven up — it was the one that was supposed to cheer you up. See some research here.
For the last several years it has been claimed that some 98% of legitimate scientists believe it is a major need to reduce CO2 output so as to stop the world from getting warmer. When Trump visited the pope 4 yers ago, the pope would not speak to him expect to hand him his anti-global warming letter he’d written, “Laudato Si” and to tell Trump to get on board to stop global warming. Trump said he would read the letter.
Trump visits the pope, and the pope does not look happy
I’m not a fan of science established by Papal dictate based on an informal poll of experts, especially here where the minority includes some of the greatest minds of the 20th century, and the poll is taken by Al Gore’s science expert, but that’s where we are when it comes to science and politics. I also find it that the pope blames the US for global warming but not China when the the majority of CO2 came from China, a country committed to increasing its use of coal. But be this as it may be — the pope doesn’t blame China for imprisoning Catholics either, most recently the editor of Hong Kong’s most widely read newspaper.
So I thought I take a step back to look at the desirability of making the world colder. Is a colder world a better world? Sad pictures of polar bears are presented in favor of the colder world, but for all I know, polar bears prefer it warm. Their numbers are increasing.
Paul McCarthy lyrics; Hey Jude.
If we had a global climate adjustment knob somewhere, a magic knob allowing you to make the world warmer or colder by turning it right, or left, I doubt the consensus would be to turn the knob left. There is no real logic to cold being good, but there is a line in “Hey Jude”: “…It’s a fool who plays it cool, by making his world a little colder.” And Svente Arrhenius, one of the great scientists of 100 years ago, said he preferred a warm earth to a cold one to avoid disease and starvation. When the climate turns colder, the result is disease and famine as crops fail and animals freeze. It’s not an option that I’d think most people would prefer. given my choice, I would prefer things a little warmer.
I should also note that our ability to fine tune the climate is not what we’d think. The world climate is chaotic, and there is no reliable knob. Historically, the most common setting is ice-age, and that’s a setting that most people really don’t like.
Most people know that aspirin can reduce blood clots and thus the risk heart attack, as shown famously in the 1989 “Physicians’ Health Study” where 22,000 male physicians were randomly assigned to either a regular aspirin (325 mg) every other day or an identical looking placebo. The results are shown in the table below, where “Myocardial Infarction” or “MI” is doctor-speak for heart attack.
Treatment
Myocardial Infarctions
No Infarction
Total
fraction with MI
Aspirin
139
10,898
11,037
139/11,037 = 0.0126
Placebo
239
10,795
11,034
239/11,034 = 0.0217
Over the 5 years of the study, the physicians had 378 MI events, but mostly in the group that didn’t take aspirin: 1.28% of the doctors who took aspirin had a heart attack as opposed to 2.17% for those with the placebo. The ratio 1.28/2.17 = 0.58 is called the risk ratio. Apparently, aspirin in this dose reduces your MI risk to 58% of what it was otherwise — at least in white males of a certain age.
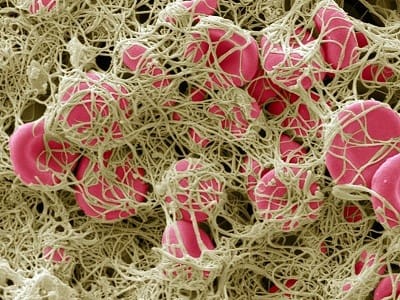
A blood clot showing red cells held together by fibrin fibers. Clots can cause heart attack, stroke, and breathing problems. photo: Steve Gschmeissner.
Further study showed aspirin benefits with women and other ethnicities, and benefits beyond hear attack, in any disease that induces disseminated intravascular coagulopathy. That’s doctor speak for excessive blood clots. Aspirin produced a reduction in stroke and in some cancers (Leukemia among them) and now it now seems likely that aspirin reduces the deadliness of COVID-19. Data from Wuhan showed that excessive blood clots were present in 71% of deaths vs. 0.4% of survivors. In the US, some 30% of those with serious COVID symptoms and death show excessive blood clots, particularly in the lungs. Aspirin and Vitamin D seem to help.
.The down-side of aspirin use is a reduction in wound healing and some intestinal bleeding. The intestinal bleeding is known as aspirin burn. Because of these side-effects it is common to give a lower dose today, just one baby aspirin per day, 81 mg. While this does does some good, It is not clear that it is ideal for all people. This recent study in the Lanset (2018) shows a strong relationship between body weight and aspirin response. Based on 117,279 patients, male and female, the Lanset study found that the low dose, baby aspirin provides MI benefits only in thin people, those who weigh less than about 60 kg (130 lb). If you weigh more than that, you need a higher dose, perhaps two baby aspirin per day, or a single adult aspirin every other day, the dose of the original doctors study.
In this study of COVID patients, published in July, those who had been taking aspirin fared far better than those who did not A followup study will examine the benefits of one baby aspirin (81 mg) with and without Vitamin D, read about it here. I should note that other pain medications do not have this blood-thinning effect, and would not be expected to have the same benefit.
While it seems likely that 2 baby aspirins might be better in fat people, or one full aspirin every other day, taking a lot more than this is deadly. During the Spanish flu some patients were given as much as 80 adult aspirins per day. It likely killed them. As Paracelsus noted, the difference between a cure and a poison is the dose.
Today, Michigan and several other, Democrat-run states are in fairly broad COVID lockdown. The justification for this is that it is “THE science”, as if this were the only possible behavior if you believe the disease is deadly and contagious. The other fellows, the governors of Republican-run states are framed as deniers of the science. Strangely enough, although this disease is most -definitely contagious and deadly, killing 209,000 Americans so far, about 0.064% of the US this year, it is far from clear that a broad lockdown is the only way to stop the disease. Sweden avoided a general lockdown, leaving its schools and restaurants open, and has seen the disease follow an almost destructive path to that of the US, with a death rate that is currently slightly lower than ours. See the excess death plot below. Sweden seems to have avoided a second, summer spike.
Mortality is Sweden vs the US; Ignore the last 2-3 weeks, it takes time for this data to be compiled
It’s bad enough for “THE SCIENCE” when you see the anti-science, no-lockdown solution provide the same result, or close. Earlier in the summer I noted that Sweden and Michigan had near the same outcome, with Sweden slightly better. It’s now the case that Sweden is doing better than the US, and much better than the D-lead lockdown states. The highest six death rate states are all D-lead, lockdown states, NY, NJ, Mass, Conn, LA, and RI, and rates are double the US average in New York and New Jersey. Perhaps the solution is a general opening, like in Sweden, but before we rush to this, it’s probably worthwhile to do some re-thinking.
Deaths per week, under 18. Any excess deaths caused by COVID-19 are invisible here, lost in the scatter.
One thing that Swedes seem to have appreciated that the US experts didn’t is that the disease hardly affects those the under 18, and that’s basically the entire K-12 student body. Sweden therefore left their K-12 schools open, while we closed ours in the US beginning in early April. At right I’ve plotted the US deaths per week for under 18 for the last three years, that is from before COVID till now. There is no evidence of excess COVID-19 deaths for this group. If anything anything, the under 18 death death rate is lower after COVID than before. This resistance of this group helps explain part of why the Swedish approach didn’t cause increased deaths. Kids in Sweden got the disease, but didn’t die of it, and likely infected their parents. The Swedes didn’t bother trying to protect everyone, but only the most vulnerable, the old people. Sweden was not completely successful at this, but we were perhaps worse, despite the general lockdown.
The excess deaths US for the 65+ bracket plotted by week of the year for 2020 (blue), 2019 (grey) and 2018 (yellow). Nearly 200,000 of the excess deaths of 2020 — the vast majority — are in this age bracket.
But what about the middle-age people that the kids would have infected, the parents and teachers. For middle age people, those in the 18-65 range, it seems to make a difference how physically fit you are, and the Swedes tend to be fit. Obesity is a big co-morbidity for this disease, and Americans tend to be obese, with things getting worse during the lockdown. Swedes also wash their hands more than we do (or so is their reputation) and they go out in the sun. There is evidence that the sun helps, and vitamin D too. A stark way of seeing how much fitness helps, for even those over 18 is to consider that, of the 1.3 million men and women of the US military, there have been only 7 COVID deaths. That is a rate 1/100 of the national average for a population that is entirely over 18. This is not to say that the death rate is quite 5 per million, (7/ 1.3 million = 5 per million), but it’s probably below 50 per million. That is to say, at least 10% of the military was likely infected.
I’m inclined to agree with Dr. Fauchi that we are not yet at herd immunity, or even close, even in states like Michigan where death rates have leveled out. Only 20% of the state shows antibodies and real herd immunity would require 75% or so. Further supporting this, our death rates are 1/2 that of New Jersey. If we were at herd immunity, that could not have happened. It is possible though that we have a sort of pseudo herd immunity, where many people in the MI population have some level of T-cell immunity. T-cells do a good job eating disease (here’s a video) but they get overwhelmed when we are exposed to more than a low dose of virus. This dose-response is common in respiratory diseases, and Dr. Fauchi has related it to T-cell immunity, though he does not speak in these directions often.
Michigan death rates to September 2020 The disease seems to be over, though only about 20% of the state shows antibodies.
T-cells can cause someone to be immune to a few viral hits, but not immune to higher doses. Assuming that’s what’s going on in MI and MA, and NJ, I’m inclined to suggest we can open up these states a bit, according to the Swedish model. That is make careful efforts to clean public transport, and encourage hand washing and surface cleaning. That we prohibit large gatherings, and we take care isolate those over 65 and protect old age homes. In the US, virtually all the deaths were of people over 65, and about half were people over 85, with men being particularly vulnerable. A heterogeneous opening of this sort has been recommended by scientists as early as March.
There are three major problems with lockdowns that keep us from all virus particles. These lockdowns kill the economy, they leave us with lousy education, and they likely leave us as at-risk for the disease later on, when the lockdown is lifted. Instead a heterogeneous opening leaves the economy running and exposes us to some small exposure, at a level that our typical level of T-cell immunity may be able to handle. Over time we expect our T-cell immunity will rise and we’ll be able to take off our masks entirely. It’s a nice route to a cure that does not require a vaccine.
The above approach requires us to trust that people will do the right thing, and requires us to accept that each may do it in his/her own way. Some may not wear the mask all the time, but may chose exercising, or staying in the sun and taking vitamin D. Some may keep to masks, or focus on hand washing. Some may try unapproved drugs, like hydroxychloroquine. We will have to be able to accept that, and our experts will have to be able to step back from running everything. In China and Russia, the experts tried run every aspect of farm production, using only science methods. The result was famine. A similar thing happened in Ireland and got a potato famine. It’s good to have expert advice, but as far as making the actual decision in each location, I put a lot of weight on the choices of those who will bear the consequences.
Robert Buxbaum September 30, 2020. As a summary, I’m for opening schools, opening most states, with masks, and hand-sanitizer, at lower occupancy ( ~50%), limiting large gatherings, going to zoom as much as possible, and isolating the aged particularly the old age homes. I also recommend vitamin D and iodine hand sanitizer.
Sweden has scientists; Michigan has scientists. Sweden’s scientists said to trust people to social distance and let the COVID-19 disease run its course. It was a highly controversial take, but Sweden didn’t close the schools, didn’t enforce masks, and let people social distance as they would. Michigan’s scientists said to wear masks and close everything, and the governor enforced just that. She closed the schools, the restaurants, the golf courses, and even the parks for a while. In Michigan you can not attend a baseball game, and you can be fined for not wearing a mask in public. The net result: Michigan and Sweden had almost the same death totals and rates, as the graphs below show. As of July 28, 2020: Sweden had 5,702 dead of COVID-19, Michigan had 6,402. That’s 13 more dead for a population that’s 20% smaller.
Sweden’s deaths pre day. There are 5,702 COVID dead since the start, out of a population of 10.63 million. There are 79,494 confirmed COVID cases, but likely a lot more infected.
Sweden and Michigan are equally industrial, with populations in a few dense cities and a rural back-country. Both banned large-scale use of hydroxy-chloroquine. Given the large difference in social distance laws, you’d expect a vastly different death rate, with Michigan’s, presumably lower, but there is hardly any difference at all, and it’s worthwhile to consider what we might learn from this.
Michigan’s deaths pre day. There are 6,426 COVID dead since the start, out of a population of 9.99 million. There are 88,025 confirmed COVID cases, but likely a lot more infected.
What I learn from this is not that social distance is unimportant, and not that hand washing and masks don’t work, but rather it seems to me that people are more likely to social distance if they themselves are in control of the rules. This is something I also notice comparing freezer economies to communist or controlled ones: people work harder when they have more of a say in what they do. Some call this self -exploitation, but it seems to be a universal lesson.
Both Sweden and the US began the epidemic with some moderate testing of a drug called hydroxychloroquine (HCQ)and both mostly stopped in April when the drug became a political football. President Trump recommended it based on studies in France and China, but the response was many publications showing the didn’t work and was even deadly. Virtually ever western country cut back use of the drug. Brazil’s scientists objected — see here where they claim that those studies were crooked. It seems that countries that continued to use the drug had fewer COVID deaths, see graph, but it’s hard to say. The Brazilians claim that the anti HCQ studies were politically motivated, but doctors in both Sweden and the US largely stopped prescribing the drug. This seems to have been a mistake.
US hospitals stopped using HCQ in early April almost as soon as Trump recommended it. Sweden did the same.
In July, Henry Ford hospitals published this large-scale study showing a strong benefit: for HCQ: out of 2,541 patients in six hospitals, the death rate for those treated with HCQ was 13%. For those not treated with HCQ, the death rate was more than double: 26.4%. It’s not clear that this is cause and effect. It’s suggestive, but there is room for unconscious bias in who got the drug. Similarly, last week, a Yale researcher this week used epidemiological evidence to say HCQ works. This might be proof, or not. Since epidemiology is not double-blind, there is more than common room for confounding variables. By and large the newspaper experts are unconvinced by epidemiology and say there is no real evidence of HCQ benefit. In Michigan and Sweden the politicians strongly recommend continuing their approaches, by and large avoiding HCQ. In Brazil, India and much of the mideast, HCQ is popular. The countries that use HCQ claim it works. The countries that don’t claim it does not. The countries with strict lock-down say that science shows this is what’s working. The countries without, claim they are right to go without. All claim SCIENCE to support their behaviors, and likely that’s faulty logic.
Hydroxychloroquine and COVID-19 fatality rates in different countries as of early June 2020. This isn’t enough to prove HCQ effectiveness, but it’s promising, and suggests that increased use is warranted, at least among those without heart problems.
Given my choice, I’d like to see more use of HCQ. I’m not sure it works, but I’m ,sure there’s enough evidence to put it into the top tier of testing. I’d also prefer the Sweden method, of nor enforced lockdown, or a very moderate lockdown, but I live I’m Michigan where the governor claims she knows science, and I’m willing to live within the governor’s lockdown.There is good, scientific evidence that, if you don’t you get fined or go to jail.
Readers of this blog know that I am not a fan of very harsh punishments for crime, in particular for crimes that have no direct victim, e.g. drug possession and sales. Prostitution is another crime with no direct victim. One could argue that society as a whole is the victim, but my sense is that punishments should be minimal and targeted, e.g. to prevent involuntary human trafficking and disease. Our current laws, depicted here, are clearly not designed for this, but there was a brief period where prostitution laws did make more sense. During the civil war, civil war, prostitution was legal and regulated to prevent disease.
In 1862, Union forces captured the southern cities of Nashville and Memphis, Tenn. Major Gen. William Rosecrans set up headquarters in Nashville. Before the war, Nashville was home to 198 white prostitutes and nine “mulatto,” operating in a two-block area known as “Smoky Row.”
By the end of 1862, Smokey row had grown and these numbers swelled to 1,500 “public women”. White southern women turned to prostitution out of poverty, largely. Their husbands were dead, or ill paid, and they were joined by recently freed slaves. Benton E. Dubbs, a Union private, reported a saying that “no man culd [sic] be a soldier unless he had gone through Smokey Row,” … “The street was about three-fourths of a mile long and every house or shanty on both sides was a house of ill fame. Women had no thought of dress or decency. They say Smokey Row killed more soldiers than the war.”
By 1863, venerial disease was becoming a major problem. The Surgeon General would document 183,000 cases of venereal disease in the Union Army alone, “…the Pocks and the Clap. The cases of this complaint is numerous, especially among the officers.”
Permit for Legal prostitution signed by Col George Spaulding.
At first General Rosecrans directed his assistant, Colonel Spaulding, to remove the women by sending them to other states, first by train, and then by boat commandeering the ship, Idaho for the purpose. The effect was horrible, not only was the ship turned back by every city, but the departure of these ladies just resulted in the appearance of a new cohort of sex-workers. By the time the Idaho had returned, Rosecrans had been relieved of command following embarrassing defeats at Chickamauga and Chattanooga . Col. Spaulding now tried a new technique to stop the plague of VD: legalized prostitution. It worked.
Women’s hospital during the war, Nashville.
For a $5/month fee a “public woman” could become a legal prostitute, or “Public Woman” so long as she submitted to monthly health inspections for a certificate of her soundness. If found infected, she was to report to a hospital dedicated to this treatment, was subject to imprisonment if she operated without the license and certificate. The effect was a major decline in sexually-transmitted disease, and an improvement (so it is claimed) in the quality of the services. The fees collected were sufficient to cover the cost of the operation and hospital, nearly.
At the end of the war, Col Spaulding and the union soldiers left Nashville, and prostitution returned to being illegal, if tolerated. One assumes that the VD rates went up as well.
George Spaulding, Congressman..
Colonel Spaulding and Maj. General Rosecrans are interesting characters beyond the above. Spaulding had entered the war as a private and rose through the ranks by merit. The rise didn’t stop at colonel. After the war, he became postmaster of Monroe Michigan, 1866 to 1870, US Treasury agent, 1871 to 1875, Mayor of Monroe, 1876 to ?, President of the board of education, a lawyer in 1878, and congressman for the MI 2nd district (Republican) 1894 -1898. He also served as board member of the Home for Girls 1885 to 1897, and postmaster of Monroe, 1899 to 1907.
William Rosecrans was a Catholic, engineer-inventor from West Point. Before the war, in 1853, he designed St. Mary’s Roman Catholic Church, one of the largest US churches at the time, site of the wedding of John Kennedy and Jacqueline Bouvier. He also designed and installed one of the first lock systems in Western Virginia. He and two partners built an early oil refinery. He patented a method of soap making and the first kerosene lamp to burn a round wick, and was one of the eleven incorporators of the Southern Pacific Railroad. After the war, he served as Ambassador to Mexico, 1868-69 and was congressman from California, 1st district (Democrat) 1880 – 1884. A true Democrat, Rosecrans could not stand either Grant or Garfield, and fought against Grant getting a retirement package.
Robert Buxbaum, June 5, 2020. There are other ways to stop the spread of sexual diseases. During the AIDS epidemic, condoms were the preferred method, and during the current COVID crisis, face masks are being touted. My preference is iodine hand wash. All methods work if they can reduce the transmission rate, Ro below 1.
I’m a fan of iodine both as a hand sanitizer, and as a sanitizer for surfaces. II’ve made gallons of the stuff for my own use and to give away. Perhaps I’ll come to sell it too. Unlike soap washing or alcohol sanitizer, iodine stays on your hands for hours after you use it. Alcohol evaporates in a few seconds, and soap washes off. The result is that iodine retains killing power after you use it. The iodine that I make and use is 0.1%, a concentration that is non-toxic to humans but very toxic to viruses. Here is an article about the effectiveness of iodine against viruses and bacteria Iodine works both on external surfaces, and internally, e.g. when used as a mouthwash. Iodine kills germs in all environments, and has been used for this purpose for a century.
With normal soap or sanitizer it’s almost impossible to keep from reinfecting your hands almost as soon as you wash. I’ve embedded a video showing why that is. It should play below, but here’s the link to the video on youtube, just in case it does not.
The problem with washing your hands after you receive an item, like food, is that you’re likely to infect the sink faucet and the door knob, and the place where you set the food. Even after you wash, you’re likely to re-infect yourself almost immediately and then infect the towel. Because iodine lasts on your hands for hours, killing germs, you have a good chance of not infecting yourself. If you live locally, come by for a free bottle of sanitizer.
For those who’d like more clinical data to back up the effectiveness of iodine, here’s a link to a study, I also made a video on the chemistry of iodine relevant to why it kills germs. You might find it interesting. It appears below, but if it does not play right, Here’s a link.
The video shows two possible virus fighting interactions, including my own version of the clock reaction. The first of these is the iodine starch interaction, where iodine bonds forms an I<sub>3</sub><sup>-</sup> complex, I then show that vitamin C unbinds the iodine, somewhat, by reducing the iodine to iodide, I<sup>-</sup>. I then add hydrogen peroxide to deoxidize the iodine, remove an electron. The interaction of vitamin C and hydrogen peroxide creates my version of the clock reaction. Fun stuff.
The actual virus fighting mechanism of iodine is not known, though the data we have suggests the mechanism is a binding with the fatty starches of the viral shell, the oleo-polysaccharides. Backing this mechanism is the observation that the shape of the virus does not change when attacked by iodine, and that the iodine is somewhat removable, as in the video. It is also possible that iodine works by direct oxidation, as does hydrogen peroxide or chlorine. Finally, I’ve seen a paper showing that internal iodine, more properly called iodide works too. My best guess about how that would work is that the iodide is oxidized to iodine once it is in the body.
There is one more item that is called iodine, that one might confuse with the “metallic” iodine solutions that I made, or that are sold as a tincture. These are the iodine compounds used for CAT-scan contrast. These are not iodine itself, but complex try-iodo-benzine compounds. Perhaps the simplest of these is diatrizoate. Many people are allergic to this, particularly those who are allergic to sea food. If you are allergic to this dye, that does not mean that you will be allergic to a simple iodine solution as made below.
The solution I made is essentially 0.1% iodine in water, a concentration that has been shown to be particularly effective. I add potassium iodide, plus isopropyl alcohol, 1%, 1% glycerine and 0.5% mild soap. The glycerine and soap are there to maintain the pH and to make the mix easier on your hands when it dries. I apply 5-10 ml to my hands and let the liquid dry in place.
While several towns have had problems with lead in their water, the main route for lead entering the bloodstream seems to be from the soil. The lead content in the water can be controlled by chemical means that I reviewed recently. Lead in the soil can not be controlled. The average concentration of lead in US water is less than 1 ppb, with 15 ppb as the legal limit. According to the US geological survey, of lead in the soil, 2014., the average concentration of lead in US soil is about 20 ppm. That’s more than 1000 times the legal limit for drinking water, and more than 20,000 times the typical water concentration. Lead is associated with a variety of health problems, including development problems in children, and 20 ppm is certainly a dangerous level. Here are the symtoms of lead poisoning.
Several areas have deadly concentrations of lead and other heavy metals. Central Colorado, Kansas, Washington, and Nevada is particularly indicated. These areas are associated with mining towns with names like Leadville, Telluride, Silverton, Radium, or Galena. If you live in an areas of high lead, you should probably not grow a vegetable garden, nor by produce at the local farmer’s market. Even outside of these towns, it’s a good idea to wash your vegetables to avoid eating the dirt attached. There are hardly any areas of the US where the dust contains less than 1000 times the lead level allowed for water.
Lead content of US soils, from the US geological survey of soils, 2014. Michigan doesn’t look half bad.
Breathing the dust near high-lead towns is a problem too. The soil near Telluride Colorado contains 1010 mg/kg lead, or 0.1%. On a dust-blown day in the area, you could breath several grams of the dust, each containing 1 mg of lead. That’s far more lead than you’d get from 1000 kg of water (1000 liters). Tests of blood lead levels, show they rise significantly in the summer, and drop in the winter. The likely cause is dust: There is more dust in the summer.
Recalled brand of curry powder associated with recent poisoning.
Produce is another route for lead entering the bloodstream. Michigan produce is relatively safe, as the soil contains only about 15 ppm, and levels in produce are generally far smaller than in the soil. Ohio soils contains about three times as much lead, and I’d expect the produce to similarly contain 3 times more lead. That should still be safe if you wash your food before eating. When buying from high-lead states, like Colorado and Washington, you might want to avoid produce that concentrates heavy metals. According Michigan State University’s outreach program, those are leafy and root vegetables including mustard, carrots, radishes, potatoes, lettuce, spices, and collard. Fruits do not concentrate metals, and you should be able to buy them anywhere. (I’d still avoid Leadville, Telluride, Radium, etc.). Spices tend to be particularly bad routes for heavy metal poisoning. Spices imported from India and Soviet Georgia have been observed to have as much as 1-2% lead and heavy metal content; saffron, curry and fenugreek among the worst. A recent outbreak of lead poisoning in Oakland county, MI in 2018 was associated with the brand of curry powder shown at left. It was imported from India.
Marijuana tends to be grown in metal polluted soil because it tolerates soil that is too polluted fro most other produce. The marijuana plant concentrates the lead into the leaves and buds, and smoking sends it to the lungs. While tobacco smoking is bad, tobacco leaves are washed and the tobacco products are regulated and tested for lead and other heavy metals. If you choose to smoke cigarettes, I’d suggest you chose brands that are low in lead. Here is an article comparing the lead levels of various brands. . Better yet, I’s suggest that you vape. There are several advantages of vaping relative to smoking the leaf directly. One of them is that the lead is removed in the process of making concentrate.
Some states test the lead content of marijuana; Michigans and Colorado do not, and even in products that are tested, there have been scandals that the labs under-report metal levels to help keep tainted products on the shelves. There is also a sense that the high cost encourages importers to add lead dust deliberately to increase the apparent density. I would encourage the customer to buy vape or tested products, only.