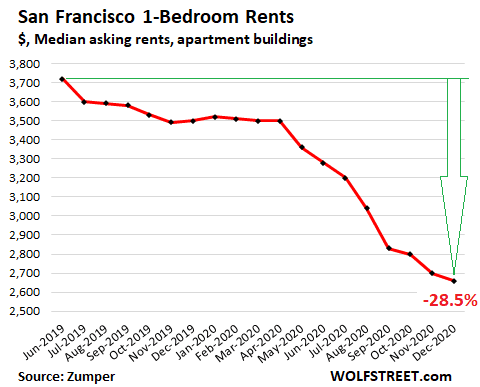
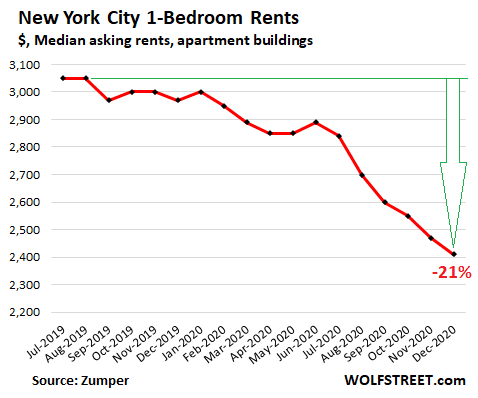
Rents in New York and San Francisco are far less expensive than before the pandemic. It’s been a boon for the suburbs, the south and the midwest, one that’s likely to continue unless Biden steps in. Before the pandemic, rent in San Francisco for a one bedroom apartment averaged over $3700 per month. New York rent was similar. People paid it because these cities offered robust business and entertainment, the best restaurants and bars, the best salons and clubs, the best music, museums, universities, and theater. New York was Wall Street, Madison Avenue and Broadway; San Francisco was Silicon valley and Hollywood. These cities were the place to be, and then the pandemic hit.
Post COVID-19, the benefits of big city life are gone, and replaced by negatives. The great restaurants are mostly gone; the museums, theaters, and salons, shut along with Hollywood. Wall Street and Madison Ave have gone on-line, as have the universities. If you can work and study from anywhere, why do it from an expensive hotbed of Corona.
People of means left the big cities with the first lockdowns. Wall Street moved on line, with offices in New Jersey, and many followed, along with college students, and hotel and restaurant workers. New York’s unemployment rate increased from 4-5% to over 9.5% today, among the highest rates in the nation, 9.5%. It would be higher if not for the departures. Crime spiked; the murder rate doubled. To keep people from leaving, landlords have lowered rents and many will now forgive a month or two of rent to keep apartments full with some rent coming in and an illusion of exclusivity. This is good for tenants, but tough on landlords.
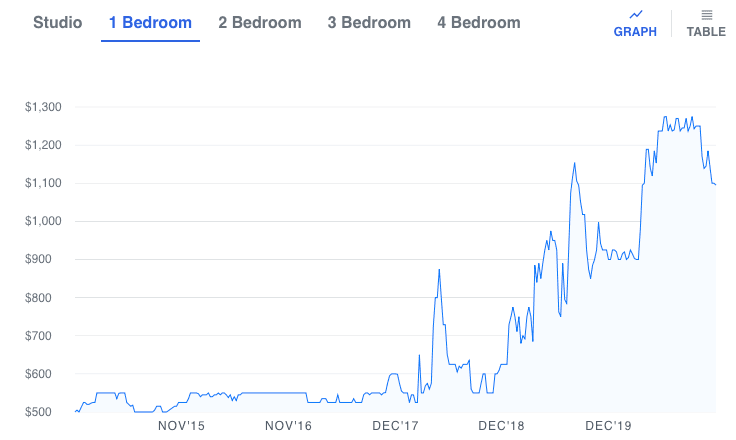
Detroit rent history, 2014 to January 2021. Rents fell a lot on election day, maybe because of Biden, or because we think the pandemic is over.
As things stand, the suburbs and smaller cities are the beneficiaries of the exodus. Among the cities benefiting the most are cities in the south and mid-west: states that are more open and are relatively low cost: Phoenix, Oakland, Cleveland, St. Petersburg, and even Detroit. Detroit’s rents were already moving up as auto manufacturing returned from Mexico, see chart. Between early 2017 and October 2020, they went from $500/month to $1250/month for a 1 bedroom apartment, according to Zumper. Detroit rents fell after election day, but are still up 20% on the year. The influx of wealthier working folk to Detroit is welcome to some, unwelcome to tenants who find their rents are raised. I think it’s is a sign of a healthy economy that people follow life-quality, and that rents follow people. Our landlords are happy, but there are a lot of Detroit renters who are not
Joe Biden has promised to step in to make things right for everyone. He promised to have the government pay people’s rent so they don’t get evicted. I presume that means paying about double to people in NY and SF as to those in Detroit. He claims he will shutter smokestack industries too, and create the good jobs of the future in computers and high tech. It’s a nice claim. I suspect it’s a bailout of big city landlords, but what would I know. I suspect that the US would be better off if Joe just sat back and let New York rents fall, while allowing Detroit to gentrify. Detroiters need not worry about rents getting too pricy here. We’ve1500 shootings per year, that 15 times more than NYC, per capita. Unless that ratio changes, Detroit will continue to be the lower rent city.
Part of the mandate to the 2020 election was to join with Europe and the rest of the western world in agreeing to stop the use of coal. It’s a low cost way to generate energy. Of course we still like to buy things, and we’ve largely turned to China, a country that still burns coal, and thus makes things cheap. The net result of this shift to Chinese goods is that China keeps building coal-fired plants while we shut ours. As it happens, China is worse than the US in terms of CO2 per output, but at least when China pollutes, we don’t see the smoke directly, and we don’t see their new coal plants at all. So we feel better buying things from China than from the US. Besides, slave labor is cheap.
From th eEconomist, December 2020.
Buying Chinese goods is good for the importers, and for the non-manufacturing consumer, at least in the short term. It has the effect of exporting jobs though, and eventually we have to support the displaced workers. It also means we don’t keep up our manufacturing technology. Long term, that affects innovation, and that starts to displace other industries. Antibiotic production has already left the US and along with it semiconductors. Still, we feel good about it since the Chinese don’t let us see the slave labor camps. We do get to see the haze of the pollution.
The Chinese expect this pattern to continue. China is building new coal-fired plants at a furious rate. Presently China has most of the world’s coal-fired power plants. Mostly these are only 4 to 12 years old, far younger than our forty year old plants China plans to build more, and keeps encouraging us to shut down ours. Even 10 years ago, China lead the world in CO2 output. And their fraction of the CO2 keeps climbing.
China is popular with the press. In part, I expect, that’s because they pay the international experts. lAlso, writers and editors are consumers industrial products, but not manufacturers. Consumers benefit from slave labor, or maybe not, but displaced American workers certainly suffer. Also, of course, the news requires pictures and personal stories to keep viewer interest. If you can’t get pictures of young protesters, like Grey Thunberg, you can get an interesting story. Our Chinese pollution is out of sight, and not in the press.
Most people know that aspirin can reduce blood clots and thus the risk heart attack, as shown famously in the 1989 “Physicians’ Health Study” where 22,000 male physicians were randomly assigned to either a regular aspirin (325 mg) every other day or an identical looking placebo. The results are shown in the table below, where “Myocardial Infarction” or “MI” is doctor-speak for heart attack.
Treatment
Myocardial Infarctions
No Infarction
Total
fraction with MI
Aspirin
139
10,898
11,037
139/11,037 = 0.0126
Placebo
239
10,795
11,034
239/11,034 = 0.0217
Over the 5 years of the study, the physicians had 378 MI events, but mostly in the group that didn’t take aspirin: 1.28% of the doctors who took aspirin had a heart attack as opposed to 2.17% for those with the placebo. The ratio 1.28/2.17 = 0.58 is called the risk ratio. Apparently, aspirin in this dose reduces your MI risk to 58% of what it was otherwise — at least in white males of a certain age.
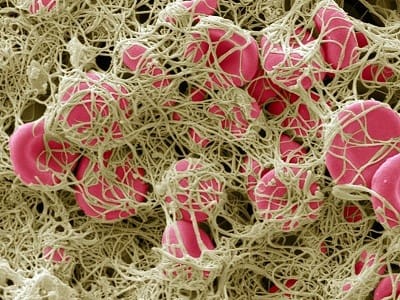
A blood clot showing red cells held together by fibrin fibers. Clots can cause heart attack, stroke, and breathing problems. photo: Steve Gschmeissner.
Further study showed aspirin benefits with women and other ethnicities, and benefits beyond hear attack, in any disease that induces disseminated intravascular coagulopathy. That’s doctor speak for excessive blood clots. Aspirin produced a reduction in stroke and in some cancers (Leukemia among them) and now it now seems likely that aspirin reduces the deadliness of COVID-19. Data from Wuhan showed that excessive blood clots were present in 71% of deaths vs. 0.4% of survivors. In the US, some 30% of those with serious COVID symptoms and death show excessive blood clots, particularly in the lungs. Aspirin and Vitamin D seem to help.
.The down-side of aspirin use is a reduction in wound healing and some intestinal bleeding. The intestinal bleeding is known as aspirin burn. Because of these side-effects it is common to give a lower dose today, just one baby aspirin per day, 81 mg. While this does does some good, It is not clear that it is ideal for all people. This recent study in the Lanset (2018) shows a strong relationship between body weight and aspirin response. Based on 117,279 patients, male and female, the Lanset study found that the low dose, baby aspirin provides MI benefits only in thin people, those who weigh less than about 60 kg (130 lb). If you weigh more than that, you need a higher dose, perhaps two baby aspirin per day, or a single adult aspirin every other day, the dose of the original doctors study.
In this study of COVID patients, published in July, those who had been taking aspirin fared far better than those who did not A followup study will examine the benefits of one baby aspirin (81 mg) with and without Vitamin D, read about it here. I should note that other pain medications do not have this blood-thinning effect, and would not be expected to have the same benefit.
While it seems likely that 2 baby aspirins might be better in fat people, or one full aspirin every other day, taking a lot more than this is deadly. During the Spanish flu some patients were given as much as 80 adult aspirins per day. It likely killed them. As Paracelsus noted, the difference between a cure and a poison is the dose.
My son works at a company called Homodeus. It’s part of 4Catalyzer, an umbrella of seven medical biotechnology companies with a staff of 300 scientists and engineers. One of the Homodeus products, still waiting FDA guidance is a COVID-19, RNA self-tester called Homodeus Detect. It tests for COVID RNA directly, not for antibodies, with tests are much faster than hospital tests, taking 45 minutes, but more complex than the unreliable test strips. So far, the Detect tests have shown no false positives or false negatives. That would suggest 100% reliable, except but there are a fair number of invalid tests. The invalid tests are lares due to the complexity, and also to the fact that you are testing snot, essentially. There is no blood-taking involved, unlike with the test strips, but just a nasal swab, and the cost is moderate, about $35 per test. However you have to do some lab work. After you swab your nose, you put the swab in a heated liquid bath where chemicals break up the snot and dissolve the shells on any viruses or pollen present. After 30 minutes, you pass the liquid onto a detector strip that contains a conjugate protein that binds to SARS-CoV-2 RNA. Your answer appears 15 minutes later as one of three lines: one for positive, one for negative, or one indicating an invalid test. Invalid tests show up more often than they like, about half the time, especially when the test is done by amateurs.
Getting an invalid test result is a downside of the current product, but I don’t think it should prevent sales. You get better at doing the test, and speed and lack of false positives and negatives is a bigger plus. It seems worthwhile to fast-track offer this test for doctors offices and hospital admissions, at least. I’d also like to see it used for airplane boarding and interstate travel, so that a person traveling might avoid the two week quarantine that many states impose. I’d certainly pay $200 or more to avoid a two-week quarantine, and if I have to do a second or third test, I’d do that too.
At least some people realize it’s a big advantage to know if you are currently infections.
Because this test measures virus RNA, and not antibodies, it indicates infection virtually as soon as you’re infected. That’s a benefit for those wishing to fly, or to meet with people, an advantage that is not lost on Elon Musk at least (see tweet). The test also shows negative as soon as the virus is gone, and that’s big. In recent months the FDA has fast-track approved an antibody indicating test from Abbott Labs, but that test has many false readings and only indicates infection several days afterward, and it does not indicate when you are no longer infectious.
The FDA has not offered to fast track this test, or any other like it for approval. They have not even indicated what sort of reporting and privacy requirements they want, so things sit in limbo, both for Homodeus, and for competing companies. Here is a story in USA today: https://www.usatoday.com/story/news/2020/07/29/fda-opens-door-rapid-home-covid-19-tests/5536528002. One big issue that the FDA is contact tracing. The FDA would like to be able to trace all the contacts of anyone who tests positive, while maintaining privacy as demanded by the 4th Amendment.
One way around the 4th amendment concerns would be to require anyone who uses the test to sign a waiver allowing the government to trace their contacts. Alternately there could be a block-chain enabled app that would come with the test. An app coms already providing a timer for when to move to the next step, and it includes a machine-vision system to help analyze dim lines on the indicator. Perhaps the FDA would accept block chain as a way to allow full reporting while maintaining privacy The FDA has yet to provide guidance on what they want, though. Without guidance or fast-track approval, things sit in limbo. Here is a scathing legal analysis from the Yale Law Journal.
You can get a free test, but have to do it at Homodeus headquarters in Guilford, Connecticut. It’s free, and results appears in about 45 minutes.. Homodeus has been manufacturing the test in quantity; if you are interested, use the following link to sign up: https://www.homodeusinc.com/research. Healthcare providers are particularly welcome.
Why did the FDA fast-track approve Abott’s antigen/ antibody test. Maybe because the tests rethought to not lead to lower mask use. Alternately, Abott has more political pull. You can read the FDA’s explanation here. In my biassed opinion the Homodeus product is good enough to fast track especially for hospitals and healthcare providers. It could save lives while allowing the economy to reopen.
Robert Buxbaum, November 15, 2020 (with massive help from Aaron M. Buxbaum)
Today, Michigan and several other, Democrat-run states are in fairly broad COVID lockdown. The justification for this is that it is “THE science”, as if this were the only possible behavior if you believe the disease is deadly and contagious. The other fellows, the governors of Republican-run states are framed as deniers of the science. Strangely enough, although this disease is most -definitely contagious and deadly, killing 209,000 Americans so far, about 0.064% of the US this year, it is far from clear that a broad lockdown is the only way to stop the disease. Sweden avoided a general lockdown, leaving its schools and restaurants open, and has seen the disease follow an almost destructive path to that of the US, with a death rate that is currently slightly lower than ours. See the excess death plot below. Sweden seems to have avoided a second, summer spike.
Mortality is Sweden vs the US; Ignore the last 2-3 weeks, it takes time for this data to be compiled
It’s bad enough for “THE SCIENCE” when you see the anti-science, no-lockdown solution provide the same result, or close. Earlier in the summer I noted that Sweden and Michigan had near the same outcome, with Sweden slightly better. It’s now the case that Sweden is doing better than the US, and much better than the D-lead lockdown states. The highest six death rate states are all D-lead, lockdown states, NY, NJ, Mass, Conn, LA, and RI, and rates are double the US average in New York and New Jersey. Perhaps the solution is a general opening, like in Sweden, but before we rush to this, it’s probably worthwhile to do some re-thinking.
Deaths per week, under 18. Any excess deaths caused by COVID-19 are invisible here, lost in the scatter.
One thing that Swedes seem to have appreciated that the US experts didn’t is that the disease hardly affects those the under 18, and that’s basically the entire K-12 student body. Sweden therefore left their K-12 schools open, while we closed ours in the US beginning in early April. At right I’ve plotted the US deaths per week for under 18 for the last three years, that is from before COVID till now. There is no evidence of excess COVID-19 deaths for this group. If anything anything, the under 18 death death rate is lower after COVID than before. This resistance of this group helps explain part of why the Swedish approach didn’t cause increased deaths. Kids in Sweden got the disease, but didn’t die of it, and likely infected their parents. The Swedes didn’t bother trying to protect everyone, but only the most vulnerable, the old people. Sweden was not completely successful at this, but we were perhaps worse, despite the general lockdown.
The excess deaths US for the 65+ bracket plotted by week of the year for 2020 (blue), 2019 (grey) and 2018 (yellow). Nearly 200,000 of the excess deaths of 2020 — the vast majority — are in this age bracket.
But what about the middle-age people that the kids would have infected, the parents and teachers. For middle age people, those in the 18-65 range, it seems to make a difference how physically fit you are, and the Swedes tend to be fit. Obesity is a big co-morbidity for this disease, and Americans tend to be obese, with things getting worse during the lockdown. Swedes also wash their hands more than we do (or so is their reputation) and they go out in the sun. There is evidence that the sun helps, and vitamin D too. A stark way of seeing how much fitness helps, for even those over 18 is to consider that, of the 1.3 million men and women of the US military, there have been only 7 COVID deaths. That is a rate 1/100 of the national average for a population that is entirely over 18. This is not to say that the death rate is quite 5 per million, (7/ 1.3 million = 5 per million), but it’s probably below 50 per million. That is to say, at least 10% of the military was likely infected.
I’m inclined to agree with Dr. Fauchi that we are not yet at herd immunity, or even close, even in states like Michigan where death rates have leveled out. Only 20% of the state shows antibodies and real herd immunity would require 75% or so. Further supporting this, our death rates are 1/2 that of New Jersey. If we were at herd immunity, that could not have happened. It is possible though that we have a sort of pseudo herd immunity, where many people in the MI population have some level of T-cell immunity. T-cells do a good job eating disease (here’s a video) but they get overwhelmed when we are exposed to more than a low dose of virus. This dose-response is common in respiratory diseases, and Dr. Fauchi has related it to T-cell immunity, though he does not speak in these directions often.
Michigan death rates to September 2020 The disease seems to be over, though only about 20% of the state shows antibodies.
T-cells can cause someone to be immune to a few viral hits, but not immune to higher doses. Assuming that’s what’s going on in MI and MA, and NJ, I’m inclined to suggest we can open up these states a bit, according to the Swedish model. That is make careful efforts to clean public transport, and encourage hand washing and surface cleaning. That we prohibit large gatherings, and we take care isolate those over 65 and protect old age homes. In the US, virtually all the deaths were of people over 65, and about half were people over 85, with men being particularly vulnerable. A heterogeneous opening of this sort has been recommended by scientists as early as March.
There are three major problems with lockdowns that keep us from all virus particles. These lockdowns kill the economy, they leave us with lousy education, and they likely leave us as at-risk for the disease later on, when the lockdown is lifted. Instead a heterogeneous opening leaves the economy running and exposes us to some small exposure, at a level that our typical level of T-cell immunity may be able to handle. Over time we expect our T-cell immunity will rise and we’ll be able to take off our masks entirely. It’s a nice route to a cure that does not require a vaccine.
The above approach requires us to trust that people will do the right thing, and requires us to accept that each may do it in his/her own way. Some may not wear the mask all the time, but may chose exercising, or staying in the sun and taking vitamin D. Some may keep to masks, or focus on hand washing. Some may try unapproved drugs, like hydroxychloroquine. We will have to be able to accept that, and our experts will have to be able to step back from running everything. In China and Russia, the experts tried run every aspect of farm production, using only science methods. The result was famine. A similar thing happened in Ireland and got a potato famine. It’s good to have expert advice, but as far as making the actual decision in each location, I put a lot of weight on the choices of those who will bear the consequences.
Robert Buxbaum September 30, 2020. As a summary, I’m for opening schools, opening most states, with masks, and hand-sanitizer, at lower occupancy ( ~50%), limiting large gatherings, going to zoom as much as possible, and isolating the aged particularly the old age homes. I also recommend vitamin D and iodine hand sanitizer.
There are two main routes for catching flu. One is via your hands and your eyes and nose. Your hands pick up germs from the surfaces you touch, and when you touch your eyes or nose passages, the germs infect you. This was thought to be the main route for infection, and I still think it is. I’d been pushing iodine hand sanitizer for some time, the stuff used in hospitals, saying that that the alcohol hand sanitizer doesn’t work well, that it evaporates.
The other route, the one touted by the press these days is via direct cough droplets, breathing them in or getting them in your eyes. Masks and face shields are the preferred protection from this route, and the claim is that masks will stop 63% of the spread. The 63% number has an interesting history, it comes from this test with infected hamsters. Hamsters are 63% less likely to infect other hamsters when they wear a mask. Of course, the comparison has some weaknesses: hamsters don’t put their fingers in their noses, nor do they rub their eyes with their hands, and hamsters can be forced to keep the mask barrier all the time — read the study to see how.
A more realistic study, or more relevant to people, in my opinion showed a far lower effect for masks, about 20%. During the HiNi flu pandemic of 2009 a group of 1437 college students at a single university were divided into three randomized groups, see the original report here. Students at a few chosen residence halls were instructed to wash their hands regularly, use sanitizer, and wear masks. Students at other halls were either told to wear masks only, or told to go on as they pleased. This was the largest group, the control. They included students of the the largest residence hall on campus. The main results appear as the graph below, Figure 1 of the report. It shows a difference of 6% or 20%, depending on how you look at things, with the mask plus hand-health group, MPHH, doing the best.
After 6 weeks of monitoring, approximately 36% of the control group had gotten the flu or some collection of flu symptoms. The remaining 64% of the residents remained symptom free. This is he darkest line above.
Of the FM Only group, the medium line above, those instructed to wear face masks only. 30% of this group showed flu symptoms, with 70% remaining symptom free. Clearly masks do help with humans, but far less than what you’d expect from the news reports.
Sweden kept the primary schools open and allows people to wear masks and social distance at they see fit. The death toll to August 1 is identical to Michigan, or slightly bette Sweden’s top virologist recommends that the US follow suit. Open up and trust people.
The group that did best was FMHH, the group who both wore facemarks and used hand health, regular hand washing plus hand sanitizer. This group reported an average of 3.5 hours per day of mask use above the control group average. This is about as good or better than I see in Michigan. Adding the hand health provided an additional 1% improvement, or a 3% improvement, depending on how you look at these things. The press claims hand health is wasted effort, but I’m not so sure. I argue that the effect was significant, and that the hand sanitizer was bad. I argue that iodine hand wash would have done better at far less social cost.
I also note that doing nothing was not that much worse than mask use. This matches with the observation of COVID-19 in Sweden. With no enforced social distancing, Sweden did about the same as Michigan — slightly better, despite Michigan closing the schools and restaurants, and imposing some of the toughest requirements for social distancing and mask use.
Other things that affect how likely you are to get flu symptoms. I find these rustles more interesting than the main face-mask result.
There were other observations from the university study that i found isignificant. There are racial differences and social differences. The authors didn’t highlight these, but they are at least as large as the effect of mask use. Asians got the flu only 70% as often as others, while black students got it 8% more often. This matches what has been seen in the US with COVID-19. Also interesting, those with a recent flu shot got flu more often; those with physical activity 13% more often. Smokers got the flu less than non-smokers and women got it 22% more often than men. The last two are the reverse with COVID-19. I could speculate on the reasons, but clearly there is a lot going on.
Why did Asians do better than others? Perhaps Asians have had prior exposure to some similar virus, and are thus slightly immune, or perhaps they used the masks more, being more socially acceptable. Why were smokers protected? It’s likely that smoke kills germs; was that the cause. These are speculations, and as for the rest I don’t know.
I am not that bothered that the students probably didn’t wear their masks 100% of the time. Better would be better, but even with mask use 100% of the time, there are other known routes that are almost impossible to remove: clothing, food, touching your face. I still think there is a big advantage to iodine hand wash, and I suspect we would be better off opening up a bit too.
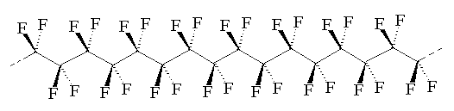
When I was eight or nine year old, I went to the 1963-64 World’s Fair in New York. Among the attractions, in “the kitchen of the future”, I saw the first version of an amazing fry-pan that was coated with plastic. You could cook an egg on that plastic without any oil, and the egg didn’t stick. The plastic was called teflon, a DuPont innovation, whose molecule is shown below.
The molecular structure of Teflon. There is an interior carbon backbone that is completely enclosed with tightly bound fluorine atoms. The net result is a compound that does not bind readily to anything else.
Years later, I came to understand that Teflon’s high-temperature stability and non-stick properties derive from the carbon-fluorine bonds. These bonds are much stronger than the carbon-hydrogen bonds found in food, and most solid, organic things. Because of the strength of the carbon-fluorine bond, Teflon is resistant to oxidation, and to chemical interaction with other molecules, e.g. in food. It does not even interact with water, making it hydrophobic and non-wetting on metals. The carbon-carbon bonds in the middle remained high temperature stable, in part because they were completely shielded by the fluorine atoms.
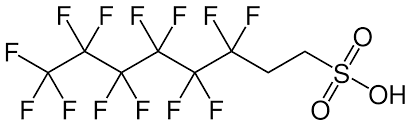
This is a PFAS. The left side is just like teflon, and very hydrophobic. The right side is hydrophilic and highly bonding to pans, and many other things like water or cotton.
But as remarkable as teflon’s non-stick properties are, perhaps the most amazing thing was that it somehow sticks to the pan. For the first generation pans I saw, it didn’t stick very well. Still, the DuPont engineers had found a way to stick non-stick Teflon to a metal for long enough to cook many meals. If they had not found this trick, teflon would not have the majority of its value, but how did they do it? It turns out they used a thin coating of a di-functional compound called PFAS, a a polyfluoro sulphonyl (or polyfluoroalkyl) substance. The molecular structure of a common PFAS, is shown above.
Each molecule of PFAS has one end that’s teflon-like and another end that’s different. The non-Teflon end, in this case a sulfonyl group, is chosen to be both high temperature stable and sticky to metal oxides. The sulphonyl group above is highly polar, and acidic. Acidic will bind to bases, like metal oxides. The surface of the metal pan is prepared by applying a thin layer of oxide or amidine, making it a polar base. The PFAS is then applied, then Teflon. The Teflon-end of the PFAS is bound to teflon by the hydrophobicity of everything else rejecting it.
There are many other uses for PFAS. For example, PFAS is applied to clothing to make it wrinkle free and stain resistant. It can also be used as a super soap, making uncommonly stable foams and bubbles. It is also used in fire-fighting and plane de-icing. Finally, PFAS is the main component of Nafion, the most common membrane for PEM fuel cells. (I can think of yet other applications..) There is just one small problem with PFAS, though. Like teflon, this molecule is uncommonly stable. It doesn’t readily decompose in nature. That would be a small problem if we were sure that PFAS was safe. As it happens it seems safe, but we’re not totally sure.
The safety of PFAS was studied extensively before PFAS-teflon pans was put on the market, but the methodology has been questioned. Large doses of PFAS were fed to test animals, and their health observed. Since the test animals showed no real signs of ill-health though some showed a slight liver enlargement, PFAS was accepted as safe for humans at a lower exposure dose. PFAS was approved for use on pans and allowed to be dumped under conditions where humans would be exposed to 1/1000 of that used on the animals. The assumption was that there would be little or no health hazard at these low exposure levels.
But low risk is not no risk, and today one can sue for even the hint of an effect though use of a class action suit. That is, lawyers sue on behalf of all the people who might have been damaged. My city was sued successfully this way for complicity in sewage over-flows. Of course, since the citizens being paid by the suit are the same ones who have to pay for the damage, only the lawyers benefit. Still, the law is the law, and at least for some judges, putting anyone at risk is enough evidence of willful disregard to hand down a stinging judgement against the evil doer. Judges have begun awarding large claims for PFAS too. While no individual can get the claim more than a tiny amount of money, the lawyers can do very well.
There is no new evidence that PFAS is dangerous, but none is needed if you can get yourself the right judge. In this regard, an industry of judicial tourism has sprung up, where class-action lawyers travel to districts where the judges are favorable. For Teflon suits, the bust hunting grounds are in New York, New Hampshire, and California, and the worst are blood-red states like Wyoming and Utah. Just as different judges promote different precedents, different states allow vastly different PFAS concentrations in the water. A common standard, one used by Michigan, is 70 ppt, 1 billion times stricter than the amounts tested on animals. This is roughly 500 times stricter than the acceptable concentratios for lead, a known poison. The standard in New York is 7 times stricter than Michigan, 10 ppt. The standard in North Carolina is 140,000 ppt, in in several states there is no legal limit to PFAS dumping. There is no scientific logic to all of this, and skeptical view is that the states that rule more strictly for PFAS than lead do so make money for lawyers. Lead is everyone in the natural environment, so you can’t sue as easily for lead. PFAS is a man-made intruder, though, and a strict standard helps lawyers sue. You can find a summary of state by state regulations here.
Any guideline stricter than about 1000 ppt, presents a challenge to the water commissioner who must measure it and enforce the law. There are tricks, though. You can use the surfactant quality of PFAS to concentrate it by a factor of 100 or more. To do this, you take a sample of river water and create bubbles. Any bubbles that form will be highly concentrated in PFAS. Once PFAS can be identified this way, and the concentrators estimated, the polluters can be held liable. Whether we benefit from the strict rulings is another story. If I were making the law for Michigan, I’d probably choose a limit about 1 ppb, but I’m not making the law. The law, as written, may be an idiot, as Bumble said, but the Law is the Law.
In terms of Michigan fishing, while some rivers have PFAS concentrators above the MI-legal limit, they are generally not far over the line. I would trust the fish in the Huron River, even west of Wixom road but I’d suggest you avoid any foam you find floating there. The PFAS content of foam will be much higher than that of the water in general.
Robert E. Buxbaum, June 30, 2020, edited July 8, 2020. There are seven compounds known as PFAS’s: perfluorooctanesulfonic acid (PFOS), perfluorooctanoic acid (PFOA), perfluorononanoic acid (PFNA), perfluorohexanesulfonic acid (PFHxS), perfluoroheptanoic acid (PFHpA), and perfluorobutanesulfonic acid (PFBS).
Brazil has decided to go its own route in response to the Corona virus pandemic. They’re using minimal social distancing with a heavy reliance on hydroxychloroquine (HCQ), a cheap drug that they claim is effective (as has our president). Brazil has been widely criticized for this, despite so far having lower death rate per million than the US, Canada, or most of Europe. In an open letter, copied in part below, 25 Brazilian scientists speak out against the politicalization of science, and in favor of their approach to COVID-19. The full letter (here). The whole letter is very worth reading, IMHO, but especially worthwhile is their section on hydroxychloroquine (HCQ), copied below.
….. Numerous countries such as the USA, Spain, France, Italy, India, Israel, Russia, Costa Rica and Senegal use the drug (HCQ) to fight covid-19, whereas other countries refrain from using HCQ as one of the strategies to contain the pandemic, betting on other controversial tactics.
Who then speaks here in the name of “science”? Which group has a monopoly on reason and its exclusive authorization to be the spokesperson of “science”? Where is such authorization found?One can choose an opinion, and base his strategy on it, this is fine, but no one should commit the sacrilege of protecting his decision risking to tarnish with it the “sacred mantle of science”.
Outraged, every day I hear mayors and governors saying at the top of their lungs that they “have followed science”. Presidents of councils and some of their advisers, and of academies and deans in their offices write letters on behalf of their entire community, as if they reflect everyone’s consensual position. Nothing could be more false.Have they followed science? Not at all! They have followed the science wing which they like, and the scientists who they chose to place around them. They ignore the other wing of science, since there are also hundreds of scientists and articles that oppose their positions and measures.
Worse, scientists are not angels. Scientists are people, and people have likes and dislikes, passions and political party preferences. Or wouldn’t they? There are many scientists, therefore, who do good without looking at whom, I know and admire many of them. But there are also pseudoscientists who use science to defend their opinion, their own pocket, or their passion. Scientists have worked and still work hard and detached to contribute to the good of humanity, many of whom are now in their laboratories, risking their lives to develop new methods of detecting coronavirus, drugs and vaccines, when they could stay “safe at home”. But, to illustrate my point, I know scientists who have published articles, some even in major journals such as “Science” or “Nature”, with data they have manufactured “during the night”; others who have removed points from their curves, or used other similar strategies. Many scientists were at Hitler’s side, weren’t they? Did they act in the name of “science”? Others have developed atom bombs. Others still develop chemical and biological weapons and illicit drugs, by design.
The Manaus’ study with chloroquine (CQ) performed here in Brazil and published in the Journal of the American Medical Association (JAMA) [1], is emblematic to this discussion of “science”. Scientists there used, the manuscript reveals, lethal doses in debilitated patients, many in severe conditions and with comorbidities. The profiles of the groups do not seem to have been “randomized”, since a clear “preference” in the HIGH DOSE group for risk factors is noted. Chloroquine, which is more toxic than HCQ, was used, and it seems that they even made “childish mistakes” in simple stoichiometric calculations, doubling the dosage with the error. I’m incapable of judging intentions, but justice will do it. The former Brazilian Health Minister Luiz Henrique Mandetta quoted this study, supported it, and based on it, categorically stated: “I do not approve HCQ because I am based on ‘science, science, science’!”.
Another study published by Chinese researchers in the British Medical Journal (BMJ) and which is still persistently used against HCQ was also at least revolting [2]. In it, the authors declared: “we administer 1,200 mg for 3 days, followed by 800 mg for 12 to 21 days, in patients with moderate to severe symptoms”. In other words, they gave a huge dosage of the drug that could reach the absurdity of 20 grams in the end, and it given was too late to patients (HCQ should be administered in the first symptoms or even earlier). And even worse, overdosing on HCQ or any other drug for severe cases is poisonous. What do you think, was it good science? The recommended dosage in Brazil, since May 20th, 2020, by the new Ministry of Health, for mild symptoms is 2 times 400 mg in the first day (every 12 hours) and 400 mg for 5 days for a total of 2.8 grams.
In other published studies, also in these internationally renowned journals such as The New England Journal of Medicine, JAMA and BMJ [3-5], once again, “problems” are clearly noted, since or the patients were randomized in irregular ways, placing older, more susceptible or most severe and hypoxemic patients in the higher (lethal) dose groups, or more men (almost 3 times more deadly by covid than women), or more black people (in the USA, black people have displayed higher mortality) and more smokers, and where most of the deaths occurred in the first days of the studies (signs that were deaths of critically ill patients, who at this stage would be more “intoxicated” than “treated” with HCQ), or they administered HCQ isolated, when it is known that it is necessary to associate HCQ at least with azithromycin. One of these studies [5] administered HCQ only on the sixteenth day of symptoms (for really early treatment, HCQ administration should be started up to fifth day), in other words, at the end of the disease, when the drug can do little good or nothing to the patient.
These studies indicate that some scientists either forgot how “science” is done or that there is a huge effort to disprove, whatever it takes, that HCQ works. How can someone or even Councils and Academies of Medicine cite such studies as the “science” of their decisions? How can that be?
On the contrary, the study published – and today with more than 3 thousand patients tested – and carried out by Dr. Didier Raoult in France [6], using the correct dosage and at the right time, with a very low mortality rate (0.4%), and the Prevent Senior’s clinical experience in Brazil – also quite encouraging – are disqualified with very “futile” arguments such as: “Didier Raoult is a controversial and unworthy researcher”, “At Prevent Senior Clinic they were not sure of the diagnosis” (but none of the hospitalized patients with clear COVID symptoms died), “Placebo effect” (what a supernatural power of inducing our mind that reduces mortality from 40% to zero, I want this placebo!), “Study performed by a health plan company” (I do not doubt that this people indeed want to save lives, because the patients were their customers who pay their bills), and similar ephemeral arguments.…
I admire the spunk of these fellows going agains the doctors, WHO. Beyond being a critique of bad research on a particular drug, it is a defense of science. Science is a discussion, a striving for truth. It is not supposed to demand blind allegiance to a few politically appointed experts. They’ve convinced me that the tests sponsored by the world health organization seem designed to show failure, and reminded me that there is rarely a one-size-fits-all for problems and all times.
I also find striking the highly critical response of my local newspapers and TV reporters. While they both like to highlight efforts by South America as they try entering the first world, with help from Bill gates and leftist politicians, they have been uniformly condemned Brazil for its non-left approach and now for use of HCQ. They want Sous Americans to think, but only if their conclusions are no different from those of their favorite, liberal thinkers.
I’m a fan of iodine both as a hand sanitizer, and as a sanitizer for surfaces. II’ve made gallons of the stuff for my own use and to give away. Perhaps I’ll come to sell it too. Unlike soap washing or alcohol sanitizer, iodine stays on your hands for hours after you use it. Alcohol evaporates in a few seconds, and soap washes off. The result is that iodine retains killing power after you use it. The iodine that I make and use is 0.1%, a concentration that is non-toxic to humans but very toxic to viruses. Here is an article about the effectiveness of iodine against viruses and bacteria Iodine works both on external surfaces, and internally, e.g. when used as a mouthwash. Iodine kills germs in all environments, and has been used for this purpose for a century.
With normal soap or sanitizer it’s almost impossible to keep from reinfecting your hands almost as soon as you wash. I’ve embedded a video showing why that is. It should play below, but here’s the link to the video on youtube, just in case it does not.
The problem with washing your hands after you receive an item, like food, is that you’re likely to infect the sink faucet and the door knob, and the place where you set the food. Even after you wash, you’re likely to re-infect yourself almost immediately and then infect the towel. Because iodine lasts on your hands for hours, killing germs, you have a good chance of not infecting yourself. If you live locally, come by for a free bottle of sanitizer.
For those who’d like more clinical data to back up the effectiveness of iodine, here’s a link to a study, I also made a video on the chemistry of iodine relevant to why it kills germs. You might find it interesting. It appears below, but if it does not play right, Here’s a link.
The video shows two possible virus fighting interactions, including my own version of the clock reaction. The first of these is the iodine starch interaction, where iodine bonds forms an I<sub>3</sub><sup>-</sup> complex, I then show that vitamin C unbinds the iodine, somewhat, by reducing the iodine to iodide, I<sup>-</sup>. I then add hydrogen peroxide to deoxidize the iodine, remove an electron. The interaction of vitamin C and hydrogen peroxide creates my version of the clock reaction. Fun stuff.
The actual virus fighting mechanism of iodine is not known, though the data we have suggests the mechanism is a binding with the fatty starches of the viral shell, the oleo-polysaccharides. Backing this mechanism is the observation that the shape of the virus does not change when attacked by iodine, and that the iodine is somewhat removable, as in the video. It is also possible that iodine works by direct oxidation, as does hydrogen peroxide or chlorine. Finally, I’ve seen a paper showing that internal iodine, more properly called iodide works too. My best guess about how that would work is that the iodide is oxidized to iodine once it is in the body.
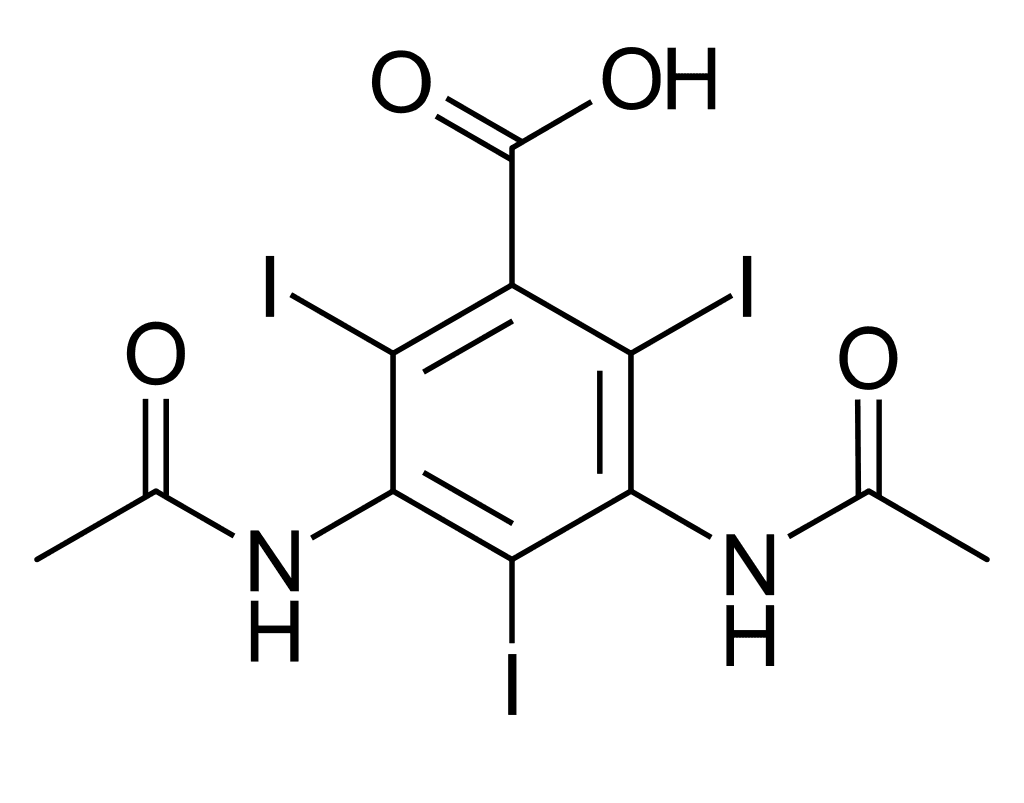
There is one more item that is called iodine, that one might confuse with the “metallic” iodine solutions that I made, or that are sold as a tincture. These are the iodine compounds used for CAT-scan contrast. These are not iodine itself, but complex try-iodo-benzine compounds. Perhaps the simplest of these is diatrizoate. Many people are allergic to this, particularly those who are allergic to sea food. If you are allergic to this dye, that does not mean that you will be allergic to a simple iodine solution as made below.
The solution I made is essentially 0.1% iodine in water, a concentration that has been shown to be particularly effective. I add potassium iodide, plus isopropyl alcohol, 1%, 1% glycerine and 0.5% mild soap. The glycerine and soap are there to maintain the pH and to make the mix easier on your hands when it dries. I apply 5-10 ml to my hands and let the liquid dry in place.
While several towns have had problems with lead in their water, the main route for lead entering the bloodstream seems to be from the soil. The lead content in the water can be controlled by chemical means that I reviewed recently. Lead in the soil can not be controlled. The average concentration of lead in US water is less than 1 ppb, with 15 ppb as the legal limit. According to the US geological survey, of lead in the soil, 2014., the average concentration of lead in US soil is about 20 ppm. That’s more than 1000 times the legal limit for drinking water, and more than 20,000 times the typical water concentration. Lead is associated with a variety of health problems, including development problems in children, and 20 ppm is certainly a dangerous level. Here are the symtoms of lead poisoning.
Several areas have deadly concentrations of lead and other heavy metals. Central Colorado, Kansas, Washington, and Nevada is particularly indicated. These areas are associated with mining towns with names like Leadville, Telluride, Silverton, Radium, or Galena. If you live in an areas of high lead, you should probably not grow a vegetable garden, nor by produce at the local farmer’s market. Even outside of these towns, it’s a good idea to wash your vegetables to avoid eating the dirt attached. There are hardly any areas of the US where the dust contains less than 1000 times the lead level allowed for water.
Lead content of US soils, from the US geological survey of soils, 2014. Michigan doesn’t look half bad.
Breathing the dust near high-lead towns is a problem too. The soil near Telluride Colorado contains 1010 mg/kg lead, or 0.1%. On a dust-blown day in the area, you could breath several grams of the dust, each containing 1 mg of lead. That’s far more lead than you’d get from 1000 kg of water (1000 liters). Tests of blood lead levels, show they rise significantly in the summer, and drop in the winter. The likely cause is dust: There is more dust in the summer.
Recalled brand of curry powder associated with recent poisoning.
Produce is another route for lead entering the bloodstream. Michigan produce is relatively safe, as the soil contains only about 15 ppm, and levels in produce are generally far smaller than in the soil. Ohio soils contains about three times as much lead, and I’d expect the produce to similarly contain 3 times more lead. That should still be safe if you wash your food before eating. When buying from high-lead states, like Colorado and Washington, you might want to avoid produce that concentrates heavy metals. According Michigan State University’s outreach program, those are leafy and root vegetables including mustard, carrots, radishes, potatoes, lettuce, spices, and collard. Fruits do not concentrate metals, and you should be able to buy them anywhere. (I’d still avoid Leadville, Telluride, Radium, etc.). Spices tend to be particularly bad routes for heavy metal poisoning. Spices imported from India and Soviet Georgia have been observed to have as much as 1-2% lead and heavy metal content; saffron, curry and fenugreek among the worst. A recent outbreak of lead poisoning in Oakland county, MI in 2018 was associated with the brand of curry powder shown at left. It was imported from India.
Marijuana tends to be grown in metal polluted soil because it tolerates soil that is too polluted fro most other produce. The marijuana plant concentrates the lead into the leaves and buds, and smoking sends it to the lungs. While tobacco smoking is bad, tobacco leaves are washed and the tobacco products are regulated and tested for lead and other heavy metals. If you choose to smoke cigarettes, I’d suggest you chose brands that are low in lead. Here is an article comparing the lead levels of various brands. . Better yet, I’s suggest that you vape. There are several advantages of vaping relative to smoking the leaf directly. One of them is that the lead is removed in the process of making concentrate.
Some states test the lead content of marijuana; Michigans and Colorado do not, and even in products that are tested, there have been scandals that the labs under-report metal levels to help keep tainted products on the shelves. There is also a sense that the high cost encourages importers to add lead dust deliberately to increase the apparent density. I would encourage the customer to buy vape or tested products, only.