Four years ago, when the average lifespan of American men was 3.1 years longer than today, the American Heart Association and the American College of Cardiology dropped the standard for normal- acceptable blood pressure for 50+ years olds from 140/90 to 120/80. The new standard of normal was for everyone regardless or age or gender despite the fact that virtually no one over 50 now reached it. Normal is now quite un-common.
By the new definition, virtually everyone over 50 now is diagnosed with high blood pressure or hypertension. Almost all require one or two medications — no more baby aspirin. Though the evidence for aspirin’s benefit is strong, it doesn’t lower blood pressure. AHA guidance is to lower a patients blood pressure to <140/90 mmHg or at least treat him/her with 2–3 antihypertensive medications.4
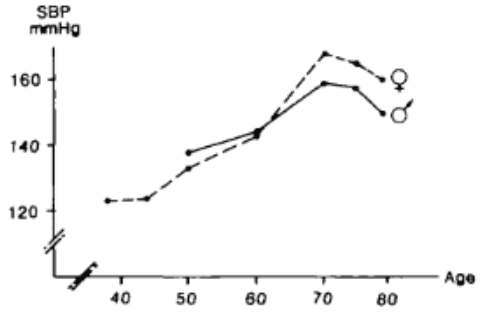
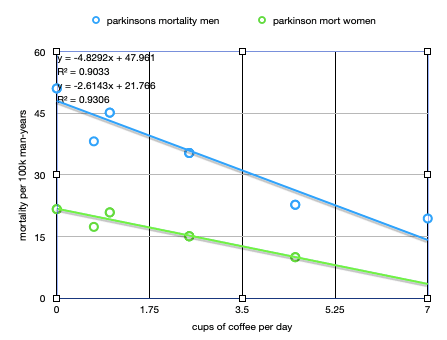
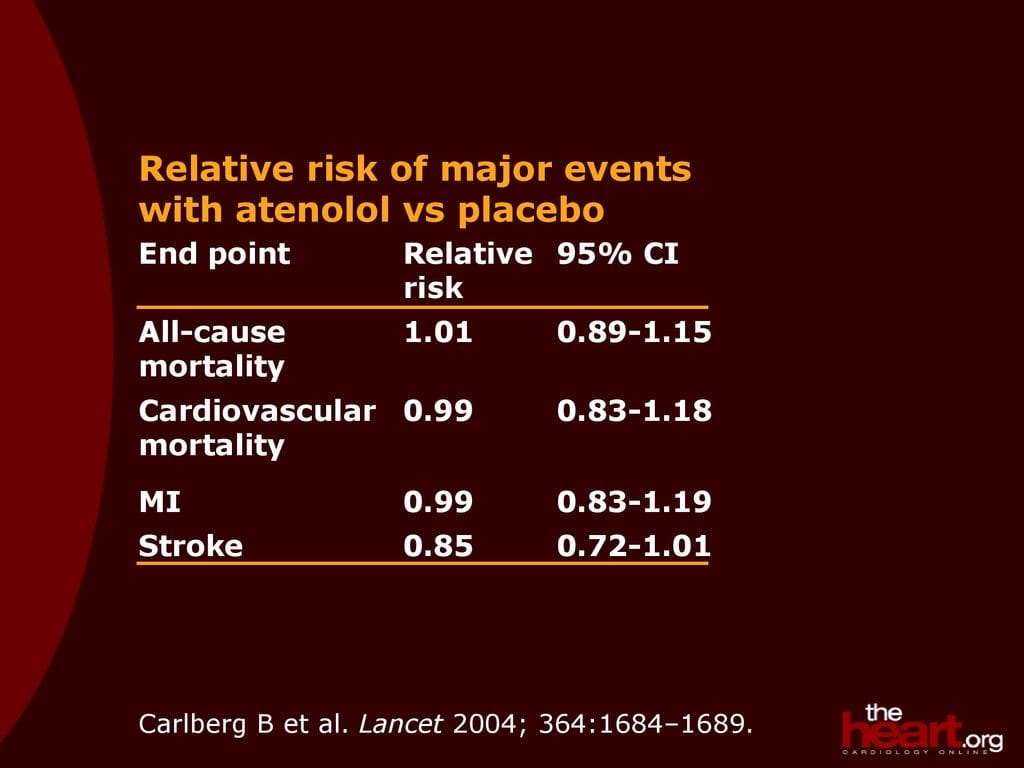
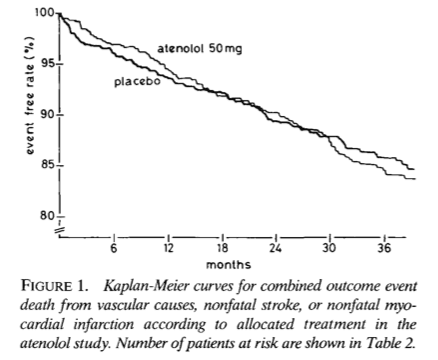
The graphs shows the average blood pressures, without drugs in a 2008 study of the longest-lived, Scandinavian populations. These were the source of the previous targets: the natural pressures for the healthiest populations at the time, based on the study of 1304 men (50-79 years old) and 1246 women (38-79 years old) observed for up to 12 years. In this healthy population, the average untreated systolic pressure is seen till age 70, reaching 154 for men, and over 160 for women. By the new standards, these individuals would be considered highly unhealthy, though they live a lot longer than we do. The most common blood-pressure drug prescribed in the US today is atenolol, a beta blocker. See my essay on Atenolol. It’s good at lowering blood pressure, but does not decrease mortality.
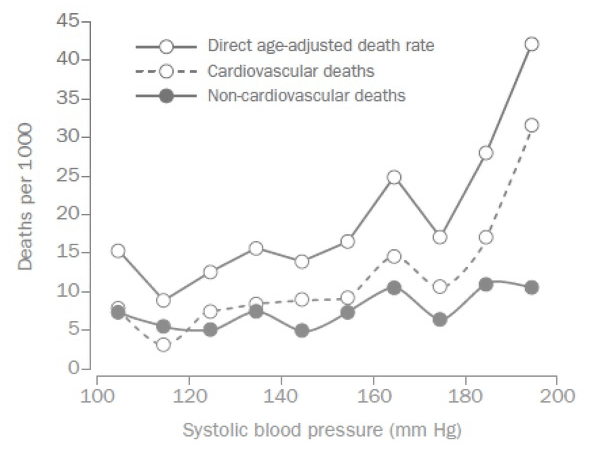
The plot at left shows the relationship between systolic blood pressure and death. There is a relationship, but it is not clear that the one is the cause of the other, especially for individuals with systolic pressure below 160. Those with pressures of 170 and above have significantly higher mortality, and perhaps should take atenolol, but even here it might be that high cholesterol, or something else, is causing both the high blood pressure and the elevated death risk.
The death-risk difference between 160 and 100 mmHg is small and likely insignificant. The minimum at 110 is rather suspect too. I suspect it’s an artifact of a plot that ignores age. Only young people have this low number, and young people have fewer heart attacks. Artificially lowering a person’s blood pressure, even to this level does not make him young, [2][3] and brings some problems. Among the older-old, 85 and above, a systolic blood pressure of 180 mmHg is associated with resilience to physical and cognitive decline, though it is also associated with higher death rate.
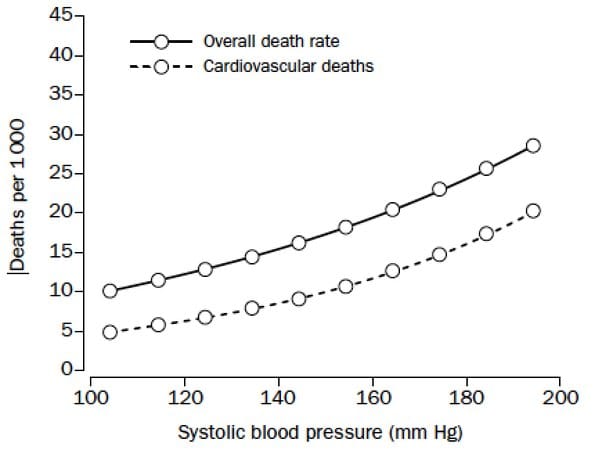
The AHA used a smoothed version of the life risk graph above to justify their new standards, see below. In this version, any blood pressure looks like it’s bad. The ideal systolic pressure seems to be 100 or below. This is vastly too low a target, especially for a 60 year old. Based on the original graph, I would think that anything below 155 is OK.
Light exercise seems to do some good especially for the overweight. Walking helps, as does biking, and aerobics. Weight loss without exercise seems to hurt health. Aspirin is known to do some good, with minimal cost and side effects. Ablation seems to help for those with atrial fibrillation. Elequis (a common blood thinner) seems to have value too, for those with atrial fibrillation — not necessarily for those without. Low sodium helps some, and coffee, reducing gout, dementia and Parkinson’s, and alcohol. Some 2-3 drinks per day (red wine?) is found to improve heart health.
I suspect that the Scandinavians live longer because they drink mildly, exercise mildly, have good healthcare (but not too good), and have a low crime rate. They seem to have dodged the COVID problem too, even Sweden that did next to nothing. it’s postulated that the problem is over medication, including heart medication.
Robert Buxbaum, January 4, 2023. The low US lifespan is startling. Despite spending more than any other developed countries on heath treatments, we have horribly lower lifespans, and it’s falling fast. A black man in the US has the same expected lifespan as in Rwanda. Causes include heart attacks and strokes, accidents, suicide, drugs, and disease. Opioids too, especially since the COVID lockdowns.